
In the 1950s, millions of people all over the world were looking for something to make them feel better. The demand for barbiturates, sleeping pills and amphetamines was huge – and growing. Most of the sedatives were barbiturates, which made people feel relaxed and euphoric, but the death toll from overdoses, deliberate and accidental, was rising.
Thalidomide promised to change all that: Marketed under the trade name Contergan in West Germany, Distaval in Britain and Talimol in Canada, it may have been the best sleeping pill ever invented: It actually cured insomnia and provided prompt, deep and natural sleep. It also relieved pain, headaches, coughs and colds. It was especially effective for pregnant women suffering from morning sickness. The manufacturer insisted there were no side effects.
In 1960, Frances Kelsey was a recently appointed medical reviewer at the U.S. Food and Drug Administration. The new drug application (NDA) for thalidomide was her second file.
"They gave it to me because they thought it would be an easy one to start on," she said. "As it turned out, it wasn't all that easy."
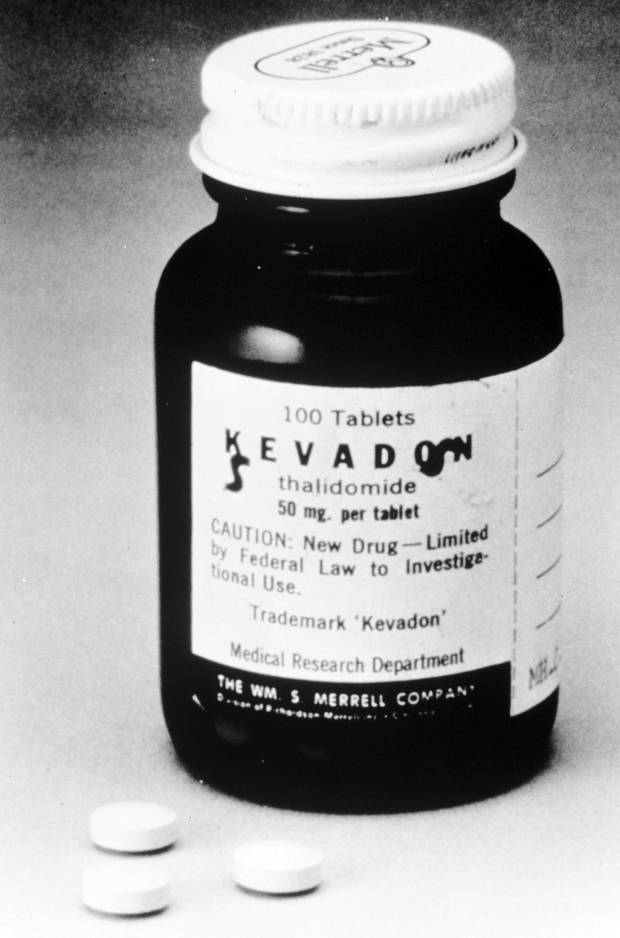
Thalidomide was marketed by the FDA in over 20 countries.
FDA file photo
Frances Oldham was born on July 24, 1914, in Cobble Hill – a village just north of Victoria on Vancouver Island. Her English father, Colonel Frank Trevor Oldham, a retired British Army officer, had married a young Scotswoman, Frances Katherine Stuart. Their daughter was one smart tomboy, graduating from high school when she was only 15. "I always knew I'd be some kind of scientist," she recalled.
Frances Kelsey received her PhD in pharmacology in 1938 from the University of Chicago. At war's end, she began medical school there.
She accepted a position with the Journal of the American Medical Association and, together with her PhD supervisor Dr. E.M.K. Geiling and her husband, Dr. F. Ellis Kelsey, published Essentials of Pharmacology. Then, in 1960, a job offer arrived from the FDA's director of the Bureau of Medicine, Dr. Ralph Smith, who, like Dr. Kelsey, was from Canada and a pharmacologist.
Dr. Kelsey, who had become an American citizen in the mid-1950s, began work in 1960 in Washington in a ratty, uncarpeted cubicle in a dingy temporary office building on the National Mall. She was appointed one of a handful of medical reviewers of new drug applications (NDAs). Dr. Kelsey didn't know it at the time, but her predecessor, Dr. Barbara Moulton, had quit the FDA in disgust because her superiors regularly overruled her.
One month after Dr. Kelsey was hired, the NDA for a drug called Kevadon, or thalidomide as it is better known, arrived at the FDA offices. The applicant was William S. Merrell Inc. of Cincinnati, an American pharmaceutical company with plans to manufacture thalidomide under licence from Chemie Grünenthal, a family-owned West German company. As it turned out, Grünenthal had a record of rushing bad and inadequately tested drugs to market. The company claimed it was impossible to overdose on the drug. This claim was untrue: Taken in syrup form, thalidomide killed laboratory animals, but Merrell kept quiet about these results. There was another bonus: Thalidomide was not addictive, or so they said.
The NDA rules required a decision from the FDA within 60 days. Merrell was so confident of speedy approval that it planned a massive marketing campaign for the beginning of March, 1961, and began to stockpile supplies.
The long-term plan was for the drug to be made available over the counter, but first the FDA had to say yes.

From April 1969, the lab of pharmaceutical company Gruenenthal, in Stolberg, West Germany. They were the makers of thalidomide, which caused thousands of babies to be born with shortened arms and legs or no limbs at all in the 1960’s.
Anonymous/The Associated Press
Under the leadership of FDA Commissioner George P. Larrick, the relationship between the regulator and the pharmaceutical industry was closer than it should have been. There was the usual wining and dining at the top, and from time to time the coziness decayed into outright criminality. One senior official was exposed in 1960 after he accepted more than $250,000 from the antibiotics industry. When the Merrell NDA arrived, three FDA employees were assigned to the file: Dr. Kelsey, the medical officer; a chemist named Lee Geismar; and a pharmacologist, Oyam Jiro. Soon after they began their investigations, Ms. Geismar and Mr. Jiro had some concerns, and Dr. Kelsey had a lot of questions.
The way the approval system worked at the FDA, if staff identified issues within the 60 days, a notice could be sent requesting further information. The company would have to submit a new NDA, and the 60-day clock would begin to run all over again. Two days before the deadline, after which approval would be automatic if she did nothing, Dr. Kelsey mailed a notice declaring the application incomplete; in her words, "the chronic toxicity data are incomplete and, therefore, no evaluation can be made of the safety of the drug when used for a prolonged period of time." She also asked for more information on the animal studies, and many other items. As one analyst has written, "Kelsey's doubts were piqued early on by the vagueness of the application and the grandiosity of the claims." Dr. Kelsey was particularly concerned about the clinical trials and wanted more detail. "My job," she said at the time, "is to pick these new-drug applications to pieces." American law allowed the experimental use of drugs while the approval process was in process. Drug companies routinely sent free samples to doctors – to begin laying the foundation for future sales. As for the patients, no informed consent was required by law.
When Dr. Kelsey asked for more information, Merrell pushed back – hard.
Because of concerns that the FDA was captive to the industry, Commissioner Larrick had recently promised Congress that pharmaceutical companies would not be allowed to contact examiners during the approval process. That did not stop Merrell: On more than 50 occasions, aggressive industry representatives visited the FDA and hounded Dr. Kelsey and the other medical reviewers. Sometimes they sent a good cop, offering assistance, and other times a threatening bad cop. Some representatives were accompanied by respected clinical investigators – window dressing, really – to bolster their case.
Company executives insisted that Dr. Kelsey was depriving the American people of an amazing drug. They complained to Dr. Kelsey's superiors that she was fussy, nitpicking, stubborn, unreasonable and obstructionist, a completely gendered critique that almost certainly would never have been applied to a man. "Most of the things they called me, you couldn't print," she said. It was clear to Dr. Kelsey that Merrell considered her "an unreasonable female." Many pharmaceutical companies applied pressure to obtain FDA approval, but "in no instances was it as severe as with this application." But still she would not budge.
Dr. Kelsey's thorough approach seems to have "put her at odds" with older members of her organization. Internal disagreements have been described as a "civil war." But Dr. Kelsey had the support of her boss – Ralph Smith – and she was not being obstinate without reason: She followed the best scientific practices. She conducted a thorough literature review, consulted colleagues and other researchers, carefully studied the underlying research design of Merrell's supporting studies, scrutinized thalidomide's chemical composition and stability, and did her best to verify Merrell's various claims.
In mid-January, 1961, Merrell resubmitted the Kevadon NDA. All the questions about the drug's metabolism, excretion, absorption levels and toxicity remained unanswered. Dr. Kelsey was not prepared to rush: It was a sleeping pill, after all, and plenty of safe brands were already available. Then, in late January or early February, she read a short letter in the British Medical Journal from a Dr. A. Leslie Florence. Titled "Is Thalidomide To Blame?" Dr. Florence reported that some patients taking thalidomide were experiencing peripheral neuritis – a painful tingling in the arms and legs.
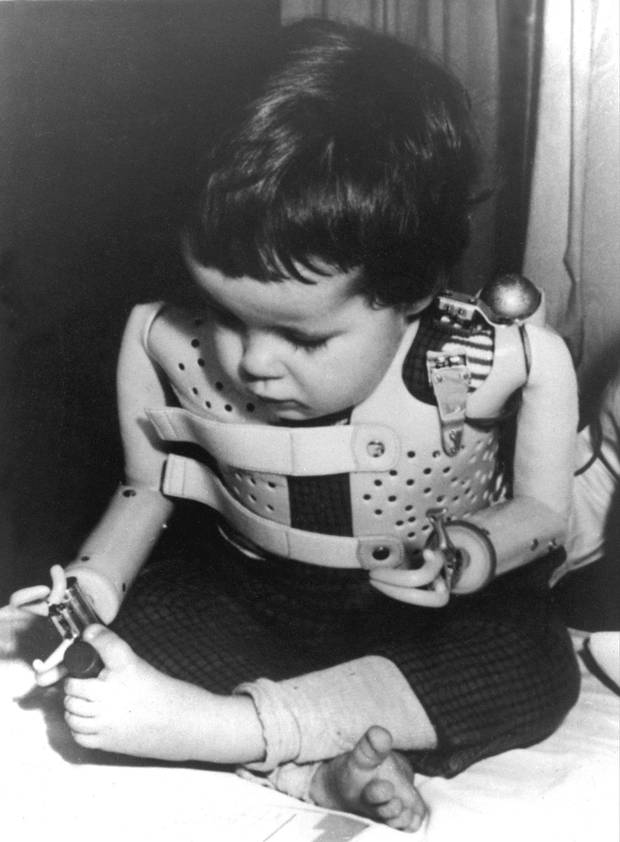
In a 1965 file photo provided by the U.S. Department of Health, a three-year-old girl, born without arms to a German mother who took thalidomide, uses power-driven artificial arms.
The Associated Press
Although a pharmacologist and a physician, Dr. Kelsey could make no sense of this report from any scientific or medical perspective. "Peripheral neuritis did not seem the sort of side effect that should come from a simple sleeping pill," she reasoned. Dr. Kelsey got some reassurance at home. Her husband was a respected scientist in his own right. He looked at the revised NDA and described it as a "collection of meaningless, pseudoscientific jargon, apparently intended to impress chemically unsophisticated readers." It was worse than bad: "I cannot believe this to be honest incompetence," he concluded. Relieved to have her suspicions confirmed, Dr. Kelsey deemed the second application incomplete.
Again she wrote Merrell asking for additional information and more proof about safety.
Dr. Kelsey soon learned that the side effects mentioned in the doctor's letter were already documented in Europe, though they had never been mentioned in the NDA. When Grünenthal's American representative was asked about them, he replied, like Sergeant Schultz in Hogan's Heroes, that he knew nothing.
"I had the feeling," Dr. Kelsey wrote after one meeting with company representatives, "that they were at no time being wholly frank with me." Merrell then made matters worse by claiming, after an investigation, including a trip to England and West Germany, that the reports about neuritis proved not to be serious, and were, Grünenthal advised, reversible; moreover, they were possibly connected to vitamin deficiencies and poor diet, not to thalidomide. The truth, however, was that the side effects were severe, widespread and directly related to the drug.
Although Dr. Kelsey had no way of knowing, by the time Dr. Florence's letter was published, Grünenthal had received hundreds of reports of severe peripheral neuritis attributable to thalidomide, and 1,500 reports of other side effects, all of which the company summarily dismissed. Privately, however, the company was worried, and with good reason. It took a baby step and ended over-the-counter sales in Germany, but it was too little and too late. Documents uncovered as part of a class-action lawsuit in Australia started by a thalidomide victim named Lynette Rowe revealed that Grünenthal's lawyers were, at the time, repeatedly warning it of a legal "avalanche coming at us." As if on cue, the West German medical press was soon filled with articles about the dangers of thalidomide. It was now revealed that doctors, including those paid by Grünenthal to test the drug, had complained from the start about its safety. In response to these complaints, Grünenthal always played dumb: "We feel obliged to say that this is the first time such effects have been reported to us" was a standard and completely untrue response. Based on Dr. Florence's letter alone, however, Dr. Kelsey had demanded all the background clinical reports and research. When Merrell failed to follow through on its promise to provide the documentation, Dr. Kelsey became convinced that thalidomide really was too good to be true.
In April, 1961, Merrell changed tack with its application for approval.
Thalidomide might have problems, company representatives advised Dr. Kelsey, but it was better than most barbiturates that were commonly used to induce sleep. It now admitted that its own studies had shown that rats could be killed by the drug. Dr. Kelsey asked the company point blank how it could submit an NDA without disclosing the evidence of neurological toxicity. In her opinion, it was impossible to approve this application: The animal and clinical studies were unpersuasive and incomplete, there was no proof the drug was safe, and information indicating other problems had been withheld.
But Merrell did not see it that way. "They thought I was nuts," Dr. Kelsey recalled. When she wrote Merrell observing that "evidence with respect to the occurrence of peripheral neuritis in England was known to you but not forthrightly disclosed in the application," the company appealed to her boss and grumbled about "libel" and the "meddlesome fool" who was standing in their way. Still Dr. Kelsey would not give in – and upped the ante.

Old photos of Dr. Kelsey at her home in 2014.
Michelle Siu/For The Globe and Mail
Just at this time the FDA was becoming interested in the effect of drugs on fetuses and had begun to develop guidelines. Dr. Kelsey knew from her time at Chicago, when working in Dr. Geiling's laboratory, that drugs affected adult rabbits and rabbit fetuses differently. She also knew that drugs could and did pass through the placental barrier. Some drugs caused malformations, or teratogen, in fetuses. When steroid hormones were prescribed in threatened miscarriages, for instance, some babies were born with heightened masculine qualities.
This was not rocket science, but established science. There were hundreds of published papers, references in leading texts and international medical conferences devoted to the phenomenon. Dr. Kelsey now asked Merrell about thalidomide in pregnancy. "Here was a drug that, given for three or four months, could cause severe neuropathy. With thalidomide, a growing infant might, perhaps, be exposed to it for five or six or up to nine months," she remarked, and so she wanted to know whether it might have an adverse effect on a child. Merrell had no answer. Apart from one study conducted during late pregnancy, the company had not even considered the question. It later turned out that thalidomide, even a single pill, caused deformities if taken between the 27th and 40th day after conception.
Testing for birth defects should have been normative. Merrell had conducted reproductive testing on several of its drugs, but not this one, having relied on Grünenthal's assurances. While Grünenthal would endlessly repeat that it followed best practices, this was not so.
The one thing Grünenthal did say that was correct was that there was, at the time, no legal obligation to conduct these tests. Maybe that is why Merrell rejected Dr. Kelsey's invitation to conduct a study, offering instead, in return for FDA approval, to put a warning on the label that thalidomide should not be taken during pregnancy and that peripheral neuritis was one possible side effect. When this offer was rejected, Merrell "ordered" Dr. Kelsey to approve the drug within one week or else, and provided some of what would soon turn out to be completely fabricated studies attesting to thalidomide's safety. Again, she stood firm: If the drug could save lives, that would have been one thing, but it was just a sedative in a market saturated with them. "The field of usefulness of the drug is such that untoward reactions would be highly inexcusable," Dr. Kelsey replied coolly.
By now a year had passed since Merrell first submitted the NDA for thalidomide in September, 1960. Formal approval had been prevented by a slim, well-mannered and shy woman who turned out to be an obstreperous and obdurate bureaucrat – at least in the manufacturer's eyes.
"Then, quite suddenly, the news came in from Europe about horrible deformities." In November, 1961, a German pediatrician, Widukind Lenz, head of the children's clinic at Hamburg University, determined that a growing number of mothers with deformed children had taken thalidomide during their first trimester – the period scientists call organogenesis, when limbs and organs are formed.
Dr. Lenz called Grünenthal and spoke to the chemist, Heinrich Mückter, who was disturbingly nonchalant. Dr. Lenz thereupon put his concerns in writing to Grünenthal, outlining the epidemic of a "certain type of deformity" that could be traced back to 1957. The one common denominator was thalidomide.
A letter from The White House to Dr. Frances Kelsey.
Michelle Siu/For The Globe and Mail
At almost this exact moment, information came in from Australia that left no doubt that thalidomide was causing serious side effects (as did private reports from the British manufacturer). The German press got hold of the story, which became big news throughout the fall of 1962. Welt am Sonntag (World on Sunday) reported that a popular sleeping drug was injuring babies. It did not have to name thalidomide – everyone knew. And so it was that Grünenthal finally agreed to withdraw the drug. Reports of massive numbers of birth defects, spontaneous abortions and stillbirths began to come in from all over the globe.
Astonishingly, Grünenthal continued international marketing until the end of January, 1963. Some countries like Canada dithered and dallied: There were 30 more victims before regulatory authorities finally woke up in March, 1962 (including some truly remarkable Canadians like Fiona Sampson, the tireless human-rights advocate who received the Order of Canada in 2015).
Around the world, in contrast to the United States, the thalidomide story was just starting. It is hard to know for sure, but perhaps as many as 10,000 people were affected in about 50 countries, not counting the thousands of spontaneous abortions and stillbirths. Many infants did not survive their first birthday. Whole families were destroyed by the guilt, shame, rage and terror. The financial burdens were overwhelming.

U.S. President John F. Kennedy presented the President’s Award for Distinguished Federal Civilian Service to Dr. Kelsey in August, 1962.
FDA
In Canada the situation was made much worse than it should have been.
Thalidomide was not ordered off the shelves until March, 1962, and it could still be found in some pharmacies as late as mid-May, three months after West Germany, England and dozens of other countries had banned its sale.
In April, 1962, notwithstanding the weight of the evidence, the head of Canada's Food and Drug Directorate mused that thalidomide approval might be reinstated. Fortunately, saner heads prevailed. Today, estimates indicate that there are about 3,000 survivors worldwide, with just less than 100 in Canada. While formally approved for sale in April, 1961, free samples of thalidomide had been given to doctors as early as 1959.
Senseless tragedy could have easily been avoided if Canadian regulators had exercised proper vigilance.
There were lawsuits and demands for justice. It was not easy anywhere; it was a pitched fight everywhere. In Britain, survivors now receive an annual pension of around $88,000 a year. In West Germany, it's about $110,000 a year. In Canada, the then minister of health, Jay Waldo Monteith, promised in 1963 to care for the victims in "the best possible manner," which apparently meant doing nothing. Canada provided a one-time payment in 1991 – a pittance – and the process was a farce. Desperate people in financial need will often compromise their legitimate claims.
Many survivors were in terrible shape. By and large, they could no longer rely on their parents – some abandoned them immediately, others struggled and did their best, but almost all are now deceased. Many of the victims were too disabled ever to work – the average annual income was only $14,000 – and most of them endured decades of grinding poverty and social isolation, fear and shame. All of them experienced a lifetime of chronic pain and physical ailments.
That changed in May, 2015, when the Conservative government of Stephen Harper, bowing to public and media pressure, and in one of the few compassionate actions in its entire 10-year term, and thanks in large part to Health Minister Rona Ambrose, announced a generous funding package. It did not go as far as the victims and their advocates had requested, but it was a long overdue step in the right direction.
The thalidomide tragedy was averted in the United States because Dr. Kelsey, alone and in the face of fierce opposition, did her job. Her perspective was educated, fresh and unique. If there had been no thalidomide crisis, the United States, with the rest of the world following, would still at some time have brought pharmaceutical regulation into the 20th century. But thalidomide created one of those moments when something had to be done. It could not be ignored in 1961-62, and it led immediately to a better and stronger regulatory system. Maybe someone else would have stopped thalidomide in the United States had Dr. Kelsey not been assigned the NDA, but, interestingly, no one else stopped it anywhere else until it was too late. Dr. Kelsey was the only person in the entire world who said no. She said no to a bad drug application, she said no to an overbearing pharmaceutical company and she said no to vested interests who put profits first. She was one brave dissenter. In the end, the question is not what made Frances Kelsey, but why aren't there more like her?
Excerpted from Why Dissent Matters: Because Some People See Things the Rest of Us Miss, by William Kaplan (McGill-Queen’s University Press, 2017). Reprinted with permission from McGill-Queen’s University Press.